Vascular Access
IN THIS LESSON
Ports— Lesson Overview
What Is a Port?
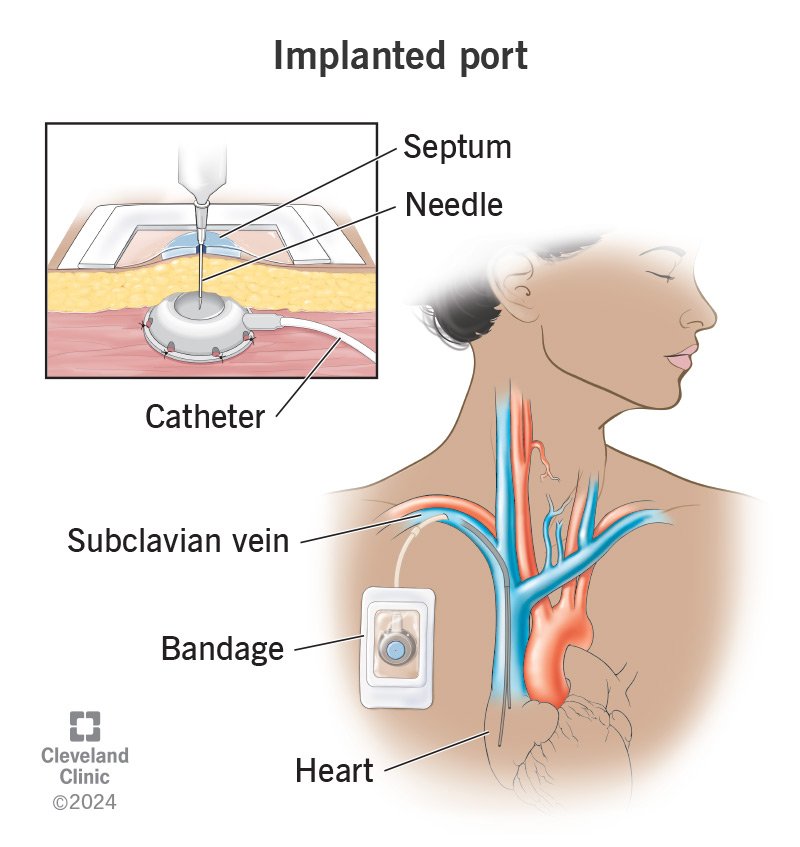
A totally implantable venous access device (TIVAD), commonly referred to as a port or port-a-cath, is a fully subcutaneous central venous access system consisting of two components: a reservoir (the port body) implanted beneath the skin, and a catheter tunneled through subcutaneous tissue into a central vein with its tip positioned at the cavoatrial junction. Unlike external catheters, the entire device sits below the skin surface, making it invisible when not in use and accessible only by puncturing the overlying skin with a specialized non-coring (Huber) needle.
Ports are designed for long-term, intermittent venous access — most commonly in oncology patients requiring repeated cycles of chemotherapy, but also for long-term antibiotics, immunotherapy, blood product transfusion, and contrast administration. Because the device is fully internalized, it carries a significantly lower infection risk than tunneled external catheters, requires minimal maintenance between access episodes (typically a monthly saline/heparin flush), and allows patients to swim, bathe, and maintain a near-normal quality of life between treatments.
In interventional radiology, port placement is performed under real-time ultrasound and fluoroscopic guidance, combining precise venous access with fluoroscopic confirmation of catheter tip position and pocket creation through a small skin incision — typically in the anterior chest wall below the clavicle. IR-guided placement has become the gold standard over surgical placement due to its superior safety profile, shorter procedure times, and reduced complication rates.
What You'll Learn in This Video
By the end of this lesson, you will be able to:
Explain what a totally implantable venous access device is, how it differs from other central venous access options such as PICCs and tunneled catheters, and when it is the preferred choice for long-term access
Identify the indications and contraindications for port placement, including oncologic and non-oncologic indications, and recognize patient or anatomic factors that may alter planning or site selection
Understand port anatomy and device components, including single versus dual lumen configurations, low-profile versus standard port bodies, titanium versus plastic reservoirs, and power-injectable port designations for high-pressure contrast administration
Recognize the relevant surface and vascular anatomy of the anterior chest wall, including the relationship between the clavicle, first rib, subclavian vein, axillary vein, and internal jugular vein, and how anatomic variation influences access site selection
Understand pre-procedural planning, including review of prior imaging for central venous patency, identification of previous access sites, and assessment of chest wall soft tissue for optimal pocket positioning
Walk through the step-by-step port placement procedure, including patient positioning, sterile preparation, local anesthesia, ultrasound-guided venipuncture, Seldinger wire advancement under fluoroscopy, pocket creation, catheter sizing and trimming, port attachment and securement, wound closure, and post-placement chest imaging
Interpret fluoroscopic landmarks used to confirm appropriate catheter tip position at the cavoatrial junction, and recognize malposition patterns including tip advancement into the right ventricle, contralateral placement, and loop formation
Identify early and late complications of port placement and use, including pneumothorax, hemothorax, arterial injury, port pocket hematoma, wound dehiscence, catheter pinch-off syndrome, port thrombosis, fibrin sheath formation, device infection, and port-a-cath fracture with embolization
Understand port access and maintenance protocols, including proper Huber needle technique, flushing and locking procedures, and the signs of a malfunctioning or infected port that should prompt IR evaluation
Recognize indications for port removal or revision, including completed treatment courses, device infection, catheter fracture, and irreversible malfunction, and understand the IR approach to explantation
-
Add a short summary or a list of helpful resources here.