Vascular Access
IN THIS LESSON
Dialysis Access — Lesson Overview
What Are Tunneled and Non-Tunneled Dialysis Catheters?
Dialysis catheters are large-bore, dual-lumen central venous catheters specifically designed to support hemodialysis by allowing simultaneous withdrawal and return of blood at the high flow rates required for effective renal replacement therapy — typically 300–500 mL/min. They represent a critical access option for patients with end-stage renal disease (ESRD) or acute kidney injury (AKI) who require immediate or temporary dialysis and do not yet have a mature arteriovenous fistula or graft.
The two principal categories differ fundamentally in their design, intended duration of use, and placement technique:
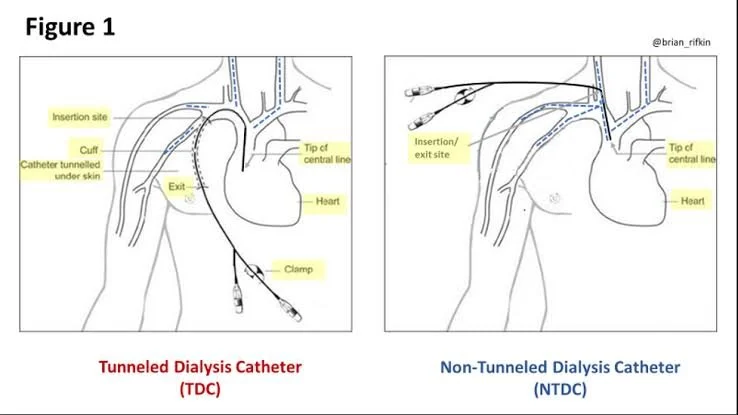
Non-Tunneled Dialysis Catheters (NTDCs) are percutaneously inserted directly through the skin into a central vein — most commonly the internal jugular or femoral vein — without a subcutaneous tunnel. They are intended for short-term use (typically fewer than 3 weeks) in the acute or critical care setting, where rapid dialysis access is needed without delay.
Tunneled Dialysis Catheters (TDCs), by contrast, are routed through a subcutaneous tunnel between the skin exit site and the venous entry point, with a Dacron cuff that anchors the catheter in the tunnel and serves as a biological barrier against ascending infection. Placed most commonly via the right internal jugular vein, TDCs are designed for long-term hemodialysis access (weeks to months) and are the preferred catheter-based bridge while a permanent access matures.
In interventional radiology, both catheter types are placed under real-time ultrasound and fluoroscopic guidance, ensuring precise venous cannulation and optimal catheter tip positioning at the cavoatrial junction.
What You'll Learn in This Video
By the end of this lesson, you will be able to:
Distinguish between tunneled and non-tunneled dialysis catheters in terms of design, intended duration of use, clinical indications, and patient population
Identify the indications and contraindications for each catheter type, including when urgent non-tunneled access is appropriate versus when a tunneled catheter should be planned
Recognize the relevant venous anatomy for dialysis catheter placement, with emphasis on the right internal jugular vein as the preferred site and understanding why vein selection directly impacts catheter longevity and function
Understand catheter design and specifications, including dual-lumen configuration, French sizing, cuff position, and the importance of tip geometry in achieving adequate flow rates
Walk through the placement technique for non-tunneled catheters, including ultrasound-guided internal jugular or femoral venipuncture, wire placement, and catheter insertion at bedside or in the IR suite
Walk through the step-by-step placement of a tunneled dialysis catheter, including vein mapping, ultrasound-guided access, fluoroscopic wire and sheath advancement, subcutaneous tunnel creation, cuff positioning, and catheter tip confirmation at the cavoatrial junction
Interpret fluoroscopic landmarks used to confirm ideal tip position and recognize malposition patterns including tip migration, coiling, and contralateral placement
Identify and manage procedural and post-procedural complications including pneumothorax, arterial injury, catheter malfunction, fibrin sheath formation, central venous stenosis, and catheter-related bloodstream infection (CRBSI)
Understand catheter exchange and removal techniques, including exchange over wire for malfunctioning catheters and the steps for safe tunneled catheter explantation
Recognize the role of dialysis catheters within the broader ESRD access planning framework, including their relationship to AV fistulas, AV grafts, and the "Fistula First" initiative
-
Add a short summary or a list of helpful resources here.